Personality of the person is something that defines them. It is the way one thinks and acts in different situations.
Personality Disorders are a group of disorders in which the personality of the individual interferes with normal functioning or poses problems in relationships. Overall, it has been seen that 2% of individuals during their lifetime suffer from Emotionally Unstable Personality Disorder. Many individuals with EUPD also have high burden of psychiatric and medical disorders.
The International Classification of Diseases (ICD) 10th edition by the World Health Organisation classifies Personality Disorders as follows:
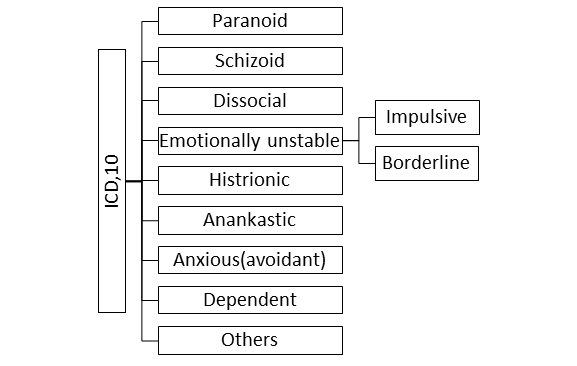
Emotionally unstable personality: As the name suggests these patients have problem in emotional regulation. A little good news and they are over joyous and a little bad news they feel rejected, sad, alienated, etc. They are further classified into two categories i.e. impulsive type and borderline type
- Impulsive type is characterised by sudden anger outburst, unstable moods, acting without thinking of the consequences and taking sudden decisions
- On the other hand, borderline type is characterised by uncertainty about self-image and disturbance in perception of others. In addition to this there may be chronic feeling of emptiness and a fear of being abandoned by others. There might be instances of multiple self-harm attempts or threats.
This is different from Complex Post Traumatic Stress Disorder (Complex PTSD) as the latter results from experiencing a specific traumatic experience (may happen more than once) and is a direct result of it. Chronic childhood adversity is common in both. In both the treatment is primarily psychotherapy but for complex PTSD a specific approach would be trying exposure‐based therapy.
In the upcoming ICD 11 there are proposed changes which align it to the recent concept of Personality Disorders in general. Two main changes are suggested i.e.
- The level of severity of dysfunction (i.e., mild, moderate, and severe) should now be evaluated in each case and
- The diagnosis is now covered under five broader domains i.e. negative affectivity, detachment, dissociality, disinhibition, and anankastia.
What are the causes of EUPD?
EUPD may arise due to one of many reasons. Biological factors like genetics are believed to play some. Usually they are believed to arise from experiences in the early childhood and trauma in the past lead to change in one’s perception and behaviour. Associations have been seen that it might also result from lack of healthy attachment figures in childhood, or the child may experience conflicts at home, this may result in experiencing trauma in childhood, death of someone near, or frequent migration.
The factors mentioned above cause a change in the thinking of the individual and eventually the person starts using unconscious defence mechanisms persistently. With time these traits are deeply ingrained as a part of persona and reflect in all behaviour.
How do I know I have EUPD?
| ICD10 Criteria
The ICD 10 describes the diagnosis of EUPD – Impulsive type if after fulfilling the general (including dysfunction criteria ) for personality disorder at least three of the following must be present, one of which is (2): (1) A marked tendency to act unexpectedly and without consideration of the consequences. (2) A marked tendency to quarrelsome behaviour and to conflicts with others, especially when impulsive acts are thwarted or criticized. (3) Liability to outbursts of anger or violence, with inability to control the resulting behavioural explosions. (4) Difficulty in maintaining any course of action that offers no immediate reward. (5) Unstable and capricious mood. For Borderline type in addition to at least two of the following should be present: (6) Disturbances in and uncertainty about self-image, aims and internal preferences (including sexual). (7) Liability to become involved in intense and unstable relationships, often leading to emotional crises. (8) Excessive efforts to avoid abandonment. (9) Recurrent threats or acts of self-harm. (10) Chronic feelings of emptiness. |
It is common to have certain traits from of the disorder as described above but that does not mean that there is a disorder. These traits may be there from childhood and they may define them. Eventually with increasing responsibilities or demanding situations may push the limits of the person and cause dysfunction. The dysfunction may be in interpersonal, social, or occupational domain which causes significant distress to the individual or the near ones. If help is sought from professionals in time further damage (developing strained relationships, having psychiatric illness, addiction etc.) can be prevented.
Is EUPD similar to mood disorder?
It is common for patients with different kinds of EUPD to suffer from co-existing mood disorders, but the two are not the same. While mood changes may be seen in patients with EUPD, like frequent fluctuations in mood, varying from extreme sadness to extreme happiness, in patients with emotionally unstable EUPD, or anxious mood particularly in social situations in anxious avoidant EUPD. They may often be difficult to differentiate from bipolar/ depressive disorder or anxiety disorders.
The difference, however, may be noted in longitudinal observation, where mood changes may show fluctuations or may be seen transiently in EUPD, while they may remain persistent and pervasive in mood disorders. Furthermore, the mood disorders usually develop in 20s or 30s and have episodic course. After the episode subsides the individual may become well-adjusted and functional.
EUPDs, on the other hand, have no definite onset as they appear in a mild form early in life, they run a more enduring course and other features apart from mood changes may be apparent to help differentiate them from mood disorders. The overall the prevalence of having mood disorders is higher among EUPD clients compared to the general population, and the presence of mood disorders in such individuals indicates a poorer prognosis.
Is there a treatment for EUPD?
There is no absolute treatment for EUPDs as personality is what defines a person. The problem in EUPDs is the maladaptive responses and inability to adapt with different situations which develops over time. Thus, the aim of treatment is not to change the person but to make them more functional and improve their adjustment with society. More than half of the individuals mature out of their EUPD with advancing age as we don’t see many borderline patients in the elderly population.
Supportive psychotherapy and crisis management are offered at the time of adverse situations. In some cases e.g. self-harm even short-term hospitalisation is warranted. Usually a long-term therapy is planned aiming at reversal of the maladaptive behavioural patterns which have developed over years.
Different therapies like psychodynamic or Cognitive-behavioural therapy are useful in decreasing these patterns. Some specific therapies like dialectic behavioural therapy in EUPD patients are based on specific problems of these individuals. Learning interpersonal skills and stress management techniques can also be helpful to them. In a few patients social skills training may be helpful in improving one’s adjustment in society. On the other hand, family therapy or couple therapy may be offered in case there are issues in family and marriage.
DBT stands for Dialectic Behavioral Therapy. The term “dialectical” here refers to balancing between two opposing forces by rational discussion. The concept of the therapy revolves around this notion of being dialectical. This therapy integrates concepts from psychoanalytical therapy (e.g. the meaning of the current behaviour being related to past) with behavioural therapy (e.g. Change in behaviour leads to improvement in psychological symptoms) to help the client deal effectively with their problems. The person is then trained to deal with the emotional pain without enacting self-injurious behaviour. The success of DBT relies on four basic skills imparted throughout the course of therapy. These are:
- Mindfulness: It simply means to be consciously aware of inner self and surroundings. This skillset helps the patient to distant themselves from their emotions and observe them from a third person perspective. Once aware, the patient can deal with these emotions in a new way.
- Distress Tolerance: As the name suggests, the client is trained to tolerate discomfort and emotional pain in a skilled manner. This brings out their ability to realise that certain distressing emotions may originate in some situations and their job is not to get overpowered by these situations. Thus, dealing more effectively in a given situations.
- Interpersonal Effectiveness: This skill aims at improving the interpersonal communication with others which includes skills like how to maintain healthy relationship, balancing the dynamic relation with others, effectively asking for something, respectfully saying “NO” etc. Thus, the client learns to reduce the extreme state faced in a relationship and keep it more balanced.
- Emotional Regulation: The therapist then actively works with the client to access, understand, and regulate their emotions. Ultimately this skillset improves positive emotions and decreases vulnerability which helps in symptoms of anxiety, anger, and depression.
Where should I seek help from?
If you or your dear ones are having symptoms mentioned above with significant distress or problems in carrying normal activities, you should consult your GP or psychiatrist. The psychiatrist will evaluate for symptoms of EUPD, whether you require treatment or not and order any investigations if required.
The cases where psychiatric admission may be indicated are – if the patient has high suicide risk, is unable to take adequate care of themselves, is a danger to others, needs intensive therapy, or there are medical/psychiatric complication.
Recommended Reading:
- Personality Disorder | Royal College of Psychiatrists. Available from: https://www.rcpsych.ac.uk/mental-health/problems-disorders/personality-disorder